
Please note that some guidelines may be past their review date. The review process is currently paused. It is recommended that you also refer to more contemporaneous evidence.
When a urine sample is required in neonates strongly suspected of having a urinary tract infection (UTI) and/or requiring antibiotics, suprapubic aspiration (SPA) of urine is the first-line investigation.
Bag urine collection is only useful to exclude infection if there is no growth of organisms.
Urine may also be collected via urethral catheter, although (particularly in males) this should only be performed by an experienced clinician.
Recommended testing
In a very ill baby, strongly suspected of having a UTI and requiring immediate antibiotics:
- Collect SPA specimen.
- Commence antibiotics even if SPA fails.
- Re-attempt collection of SPA as soon as possible.
- Bag urine specimen is totally unreliable in this instance.
In a baby strongly suspected of having a UTI and requiring antibiotics, but not immediately:
- Collect SPA specimen.
- If SPA unsuccessful, retry after one hour.
- Consider use of ultrasound to aid sample collection.
- Defer antibiotic therapy until SPA obtained, but do not await the result.
- Bag urine specimen is unreliable.
In a baby with an illness that might be a UTI but not immediately requiring treatment:
- Collect SPA specimen.
- If SPA unsuccessful, collect bag urine specimen.
- If bag urine specimen result equivocal, re-attempt SPA specimen and await the result.
- If bag urine specimen strongly suggests UTI, collect SPA specimen and commence antibiotics.
- Adjust therapy when SPA result known.
Suprapubic aspiration of urine (SPA)
Indications for SPA
Indications for SPA include:
- urine sampling
- relief of obstruction (rarely) a suprapubic catheter is a better option in this setting.
Equipment required for SPA
Equipment includes:
- 2 mL or 5 mL syringe
- 25 g or 23 g needle
- skin preparation
- sterile specimen container
- assistant to stop baby moving/extending legs
- consider use of ultrasound to guide attempt (particularly if failed already).
This procedure should be undertaken by a senior clinician, if possible.
Consider baby’s need for pain relief including the possible use of:
- application of EMLA (0.5-1 g) to proposed site 60-90 minutes before procedure
- use of oral sucrose, prior to procedure
- subcutaneous infiltration of lignocaine.
Procedure for SPA
Follow this procedure when collecting a SPA urine sample:
- Position baby supine. Hold legs in frog-like position.
- Check baby has not just voided.
- Wash hands.
- Use no touch technique.
- Prepare skin and allow to dry.
- Attach needle to syringe.
- Insertion site is 1 cm above the symphysis pubis, strictly in midline.
- Advance the syringe whilst applying minimal negative pressure.
- Aim is at 90 degrees to skin straight in (bladder is an abdominal organ in a baby).
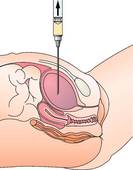 Figure 1: Needle position for SPA
Figure 1: Needle position for SPA
- Do not advance any further once urine is obtained to avoid trauma to the posterior bladder wall.
- Remove needle and apply pressure until bleeding has stopped.
- Decant into suitable container.
- If unsuccessful, alter angle by about 10-20 degrees and advance again, keeping in midline.
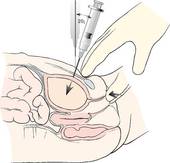 Figure 2: Altered needle position for SPA
Figure 2: Altered needle position for SPA
- If no urine is obtained after two adjustments of aim, it is likely that bladder is empty.
- Wait 45-60 minutes, ultrasound the bladder and try again.
Interpretation of SPA results
Issues to note when interpreting SPA results:
- Any leucocytes cells detected on SPA are regarded as abnormal.
- Any growth in an SPA is theoretically abnormal unless it is clearly a contaminant (for example, Staph epidermidis or heavy mixed growth of faecal bacteria.
- There is no limit to the red cell count due to the difficulty in distinguishing traumatic bleeding from true haematuria.
Bag urine collection
Indications for bag urine collection
Indications for collection of bag urine include:
- failed SPA
- low index of suspicion of UTI
- infant not requiring antibiotics
- collection of urine for purposes other than exclusion of bacterial infection (for example, analysis of specific gravity, glucose, protein).
Procedure for bag urine collection
Preparation and procedure:
- Wash area to which bag is applied with soap and sterile water, rinse with sterile water and dry.
- Apply the bag with a no touch technique (using sterile gloves).
- Remove only the bottom half of the adhesive patch first, taking care not to contaminate the inside of the bag.
- Begin application at the perineum. The narrow semi-circular bridge on the adhesive patch will prevent contamination from faeces and help position the bag correctly.
- Work from the perineum outwards, gently smoothing upward to complete the application.
- Remove the bag as soon as urine is passed and transfer the urine to the sterile specimen jar by snipping the corner of the collection bag.
Interpretation of bag urine results
The results are only useful for exclusion of infection if no growth has occurred.
Results are not useful if:
- pure growth
- mixed growth of ≥ 100,000 bacteria
- infant is already on antibiotics.
A UTI should never be diagnosed or treated on the basis of a bag urine specimen alone.
Microscopy on bag urine is not warranted, a dip-slide (urinalysis) is more useful.
Finger tap method
Follow this procedure to collect a urine sample using the finger tap method:
- Clean genital area with normal saline or water
- Ensure baby has not just passed urine
- Tap gently with two fingers just above the pubic bone.
- Tap once per second for a minute, then rest a minute
- Continue this cycle until urine appears.
The average time of micturition is 5.5 minutes. (The longest waiting time recorded is 20 minutes.)
More information
Royal Children's Hospital Melbourne parent fact sheets:
Get in touch
Version history
First published: August 2013
Review by: August 2016