On this page
When patients are unexpectedly harmed or die, a review team comes together to find out what happened, why, and how to prevent it from happening again. We help you learn from these events and near misses.
Statutory duty of candour
From November 2022, public and private hospitals will be required to:
- apologise to any person seriously harmed while receiving care
- explain what went wrong
- describe what action will be taken and improvements put in place.
These requirements come with legal protections around health service apologies and clinical incident reviews. We are developing resources to help health services prepare for and implement duty of candour. Read more about these changes.
Resources for involving impacted consumers
Healthcare patients and their families/carers who have been impacted by serious adverse patient safety events are entitled to play a role in internal review processes that seek to understand how their harm occurred.
By involving impacted consumers in adverse event reviews, a fuller understanding of contributing factors can be gained, which leads to more accurate and robust findings, and better system improvements.
In partnership with health services and consumers, we have developed a set of resources that can be used during the review process.
- Consumer involvement following a SAPSE: a 9-step guide
- Consumer & community fact sheet: What happens after patient harm?
- Next Steps Pamphlet
Rachel's story
Rachel’s Story is an example of how close engagement between a health service and an impacted consumer added significant value to the review process, produced meaningful improvements, and restored the relationship between the health service and the consumer.
Policy and guideline
Our Adverse Patient Safety Events policy provides in scope Victorian health services with the requirements, accountabilities and definitions relevant to responding to all types of adverse patient safety events. An accompanying guideline has been published to support health services in enacting the policy.
The policy was updated in 2023 to incorporate guidance for managing all types of adverse patient safety events, and amendments to the Health Services Act 1988. The policy also now includes reference to the Victorian Duty of Candour Guidelines, and Protections for serious adverse patient safety event review requirements.
The key principles guiding the development of the Adverse Patient Safety Events policy and guideline include a strong focus on learning and improvement, leadership engagement, just culture and systems thinking, and compassionate consumer engagement.
The policy provides health services with:
- key definitions related to adverse event management
- notification requirements for sentinel events
- expectations and accountabilities of health services and Safer Care Victoria when responding to adverse events, including the identifying, reporting, notifying, reviewing and monitoring of these adverse events.
The policy was updated in 2023 to incorporate guidance for managing all types of adverse patient safety events, and amendments to the Health Legislation Amendment (Quality and Safety) Bill 2021. The policy also references the Victorian Duty of Candour Guidelines, and Protections for serious adverse patient safety event review requirements.
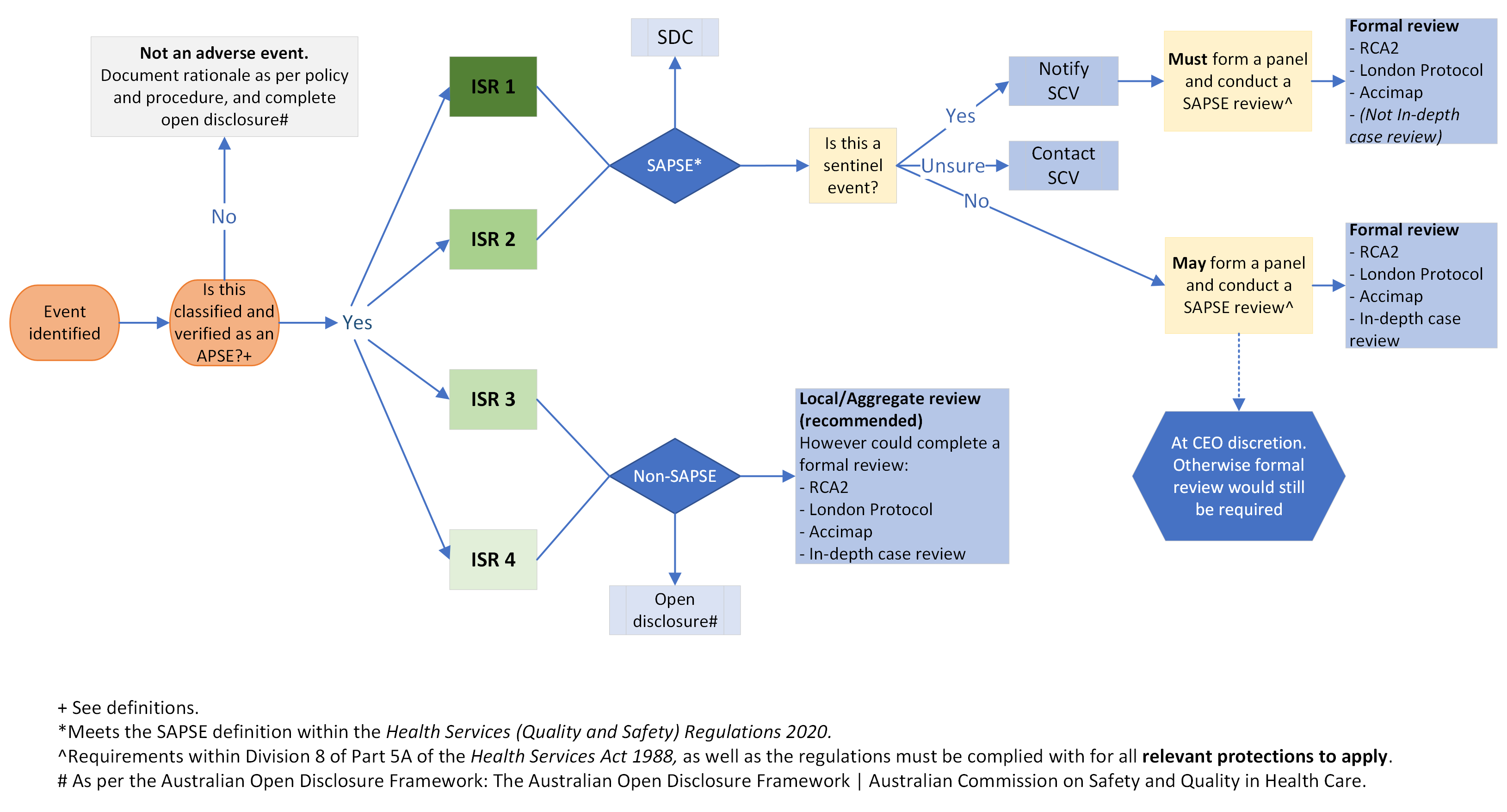
Figure 1: Provides a high-level overview of adverse event reporting and review accountabilities for all levels of adverse patient safety events.
The guideline provides health services with supporting information to enact the policy and respond to adverse patient safety events. It provides hands-on guidance on the review and improvement process, including the following elements:
- setting up and planning the review process
- forming the review team
- gathering evidence
- developing a timeline
- analysing the data
- developing findings, recommendations and action plans
- monitoring recommendations.
Read more tips on reviewing an adverse patient safety event.
You can provide feedback on the policy and guideline to help us with future revisions.
Helping you find review team members
- For external reviewers, our PEER platform will connect you with an independent member for your review team.
- For consumer members, download our guide to working together with consumers to review adverse patient safety events.
Tools and resources
Fact sheets
These fact sheets provide an introductory overview on key topics relating to adverse patient safety events. They support health services to identify, report, classify, review and learn from adverse patient safety events. The fact sheets are in line with training content, guidelines and policies developed by SCV.
Just Culture
A just culture encourages balanced accountability between organisations and individuals, and applies systems-thinking principles to allow fair and just responses to adverse patient safety events. This fact sheet helps you understand how a just culture can help you achieve positive outcomes for consumers and your organisation.
Download the Just culture fact sheet
Leadership and safety culture
Safety culture refers to an ongoing organisational commitment to safety by all staff within an organisation. This fact sheet outlines the role that organisational leaders play in building, maintaining and promoting the principles of a safety culture within their organisation.
Download the Leadership and safety culture fact sheet
Cognitive bias
Understand what cognitive biases are and how they can affect both the reviewers of adverse patient safety events and the people involved in the event that is being reviewed.
Download the Cognitive bias fact sheet.
Human factors
‘Human factors’ is the study of the interaction between people and the systems they work in. Human factors also refer to a range of systems factors (e.g. governmental, organisational, environmental) that influence human performance. This fact sheet will help you understand how human factors contribute to adverse events and helps you undertake a fair review process.
Download the Human factors fact sheet
Interviewing for adverse event reviews
Interviews are a key source of evidence to understand what contributed to adverse patient safety events. This fact sheet will help you prepare for interviews and use good interviewing principles to reduce interviewer bias.
Download the Interviewing for adverse event reviews fact sheet
Guidance Documents
This guide provides review teams with some practical tips on how to create, share and store documentation collected as part of Adverse Patient Safety Event Reviews. The information provided in this document is underpinned by the principles of Just Culture.
Download Adverse Patient Safety Event Review management guide
Developing recommendations
This guide provides review teams with practical tips on developing recommendations, what to be aware of and ensuring owners are engaged in development. It outlines how to validate recommendations against the findings and how to measure outcomes.
Download Developing recommendations
Tools
COVID-19 deaths in hospitals review tool
We have developed a systems-focused rapid tool for the review of COVID-19-related adverse events in healthcare settings. The tool guides reviewers through the basic steps of undertaking an adverse event review to examine what happened, how it happened and why it happened. Find out more and download the tool.
Maternal and Child Health Systems – Focused review tool
Maternal and Child Health (MCH) services are predominantly managed and operated by local government. Local governments do not fall under the Health Services Act 1988 (Vic) and are therefore not covered by the relevant protections when a serious adverse patient safety event (SAPSE) review is undertaken. The MCH Systems focused review tool provides MCH services with a systematic approach to client case reviews.
Download the MCH Systems focused review tool
In-depth case review tool
The in-depth case review (IDCR) tool assists health services to use a structured, systems-based approach to reviewing adverse patient safety events (APSE).
The IDCR tool is systems-focused, which means it supports reviewers in applying a systems lens when identifying factors that contributed to the adverse event occurring. The tool aligns with contemporary safety science which demonstrates that adverse events in complex systems like healthcare result from multiple interacting factors. More information on when and how to use the tool can be found in the APSE policy and guideline.
View the in-depth case review (IDCR) tool
Falls review tool
The Falls Review Tool is available for health services to use, accompanied by a user guide, which contains instructions on how to use the tool for a sentinel event.
The tool assists health services to:
- understand their current risk in relation to falls prevention
- streamline the review process
- use a human factors (systems thinking) approach to reviewing falls.
- strengthen recommendations resulting from the review of falls-related adverse events.
Health services are encouraged to familiarise themselves with the updated sentinel event guidance relating to falls.
View the Falls Review Tool